Psychological Issues around Death and Dying
Quality of Life
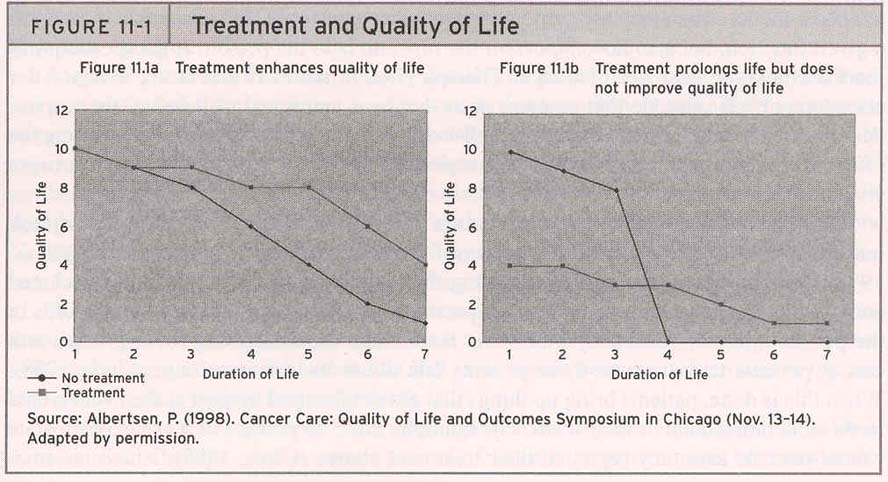
Quality of life pertains to the level of physical, cognitive, emotional and social functioning for a person and the value they place on them. Also of interest here is the effect of the disease and the treatment on these aspects of everyday living.
What rises is a trade off between the effects of the disease, treatment and one's acceptable level of functioning and impairment.
The tradeoff between
duration and quality of life
is seen where treatment may lead to some
loss of functioning while (hopefully) adding to longevity. Figure
<F11-1.jpg>![]() shows this tradeoff where treatment that
prolongs life but does not improve quality of life may not be seen favourably by
the patient.
shows this tradeoff where treatment that
prolongs life but does not improve quality of life may not be seen favourably by
the patient.
Quality of life as a subjective phenomenon
Quality of life is to be judged by the person in question. As such subjective experience of what is important in life matter. In psychology a phenomenological perspective is taken to understand subjective experience.
Hospice and palliative care treatments are given to reduce pain and suffering during terminal illness
Right to die issues emerge here again where the individual whose quality of life is seriously impaired may choose death over a degraded life.
A living will and DNR (Do Not Resuscitate) orders are issues that people are encouraged to set up in advance to ensure that their family members do not have to decide when the time comes.|
Likewise becoming and organ donor also needs to be set up in advance to lighten the load of close relatives when they are experiencing a great deal of stress and uncertainty.
Death and Dying
Patients reaction
to death
Elizabeth Kubler-Ross (1969)
outlined the typical stages of reaction to death:
1) Denial where one tends to not take the news
seriously or hopes for a mistake or error
2) Anger comes next where and one looks for someone
or somewhere to place the blame.
3) When chronic conditions are involves one
may adopt a position of Bargaining for more time, perhaps waiting for a cure or
something good to turn around one's (or one's loved one's) fate.
4)
Depression may settle in before one comes to a
state of
5)
Acceptance emerges next where death may be
seen in a more favourable light, perhaps as relief.
Table 11-3 outlines
this framework of stages <T11-3.jpg>![]() EG.
EG.
Bereavement and grief - Many terminally ill patients will be concerned about their family and friends who will undergo bereavement (the loss of a loved one) and experience grief.
As seen earlier in the course those undergoing bereavement may be at higher risk for depression, substance abuse, and various other medical problems.
Many people will also have higher mortality rates, particularly when aging people lose a spouse of many years.
Personal or group therapy may be used to help them through their difficult times.
{kind=link}
{kind=link}