Introduction
What is Health Psychology: Yesterday and Today
Overview
What
is Health psychology?
Methods and perspectives in psychology
Early
History
The
development of health psychology as a discipline
Applying
the principles of behaviorism to health
Why
has Health psychology come into prominence?
Multiple perspectives are
needed
Health
Psychology today
A biopsychosocial Approach
Working
in health Psychology
Clinical and counseling
psychologists
International Health Psychology
Marks, Murray, Evans & Estacio (2011) present several models of health,
including a historical account of its philological roots. The term arises from
old English and Old German terms of Hale, Whole, Holy and Heil or Hail. These
gave rise to the greeting "Hello". Here one can see the interest in wholeness,
being un harmed or morally good.
They
present the ideas of Galen (CE129-200)on health based upon his system of humours
![]()
Marks et
al. present more modern conceptions that include need satisfaction as seen in
Maslow's (1943) hierarch of needs with an emphasis on agency, autonomy and
spirituality.
![]()
Doyal &
Gough (1991) expand on this suggesting that there are 11 intermediate needs.
1.Adequate nutritional food and water 7.Significant
primary relationships with others
2.Adequate protective housing
8.Physical security
3.A safe environment for working
9.Economic security
4.A safe physical environment
10.Safe birth control and child-bearing
5.Appropriate healthcare
11.Appropriate basic and cross-cultural education
6.Security in childhood
Ultimately they introduce the notion that our culture and values will determine our notions of Health and other psychological abilities.
Most "western" notions of health focus on individualism and the "medical model" of disease without little regard for environmental (i.e. toxic or obesogenic) qualities.
Alternatively one might consider a more communitarian approach that include social justice, political and power issues.
What
is Health psychology?
Health psychology involves psychology's primary role in the science and profession of behavioural medicine and health care practices, disease development, treatment and prevention.
Typically
health psychology makes use of the same methods and perspectives of general
psychology.
Psychology is built upon the hypothetical deduction model of theory and research. This means that psychologists work to develop theories that give rise to specific hypotheses about the outcomes of experiments or research studies.
Statistical tools are used to
help make decisions about hypotheses and theories through a process called
inferential statistics. As such no
theory is ever really proven (only falsified) but is accepted or acknowledged as probable based
upon the likelihood that similar results could occur due to chance or random
variation in the
sample.
Theories
and models abound, but often are presented in a piecemeal fashion where few or
no grand or over arching theories exist. As
such we have many many “theories” that are applied to various aspects of
human behaviour and psychology.
Scientific perspectives are also accepted by psychologists and other scientists as “givens” that guide their thinking and provide a framework for their research and models.
Multiple perspectives exist within psychology, each providing a ‘paradigm’
for what is the nature of reality and understanding
what counts as evidence.
When two or more competing models of explanation come head to head, proponents of each attempt to make the case for their theory, like barristers making a case in a court of law.
As in that context, the rules of decision making are also human products where there may be debates over the rules of evidence as well as the results.
Marks et al discuss evidence based research, which has become prominent in resent years, but point out that it too is biased with assumptions, values and limitations in developing "knowledge".
These types of practices are judged to be sound based upon the assumptions of epistemology and methodology.
Critical thinking is important, as well as a readiness to consider alternate models as correct.
As such, Marks et al point out that a cross-cultural approach might better suited for understanding Health Psychology insofar as our notions of health and healing are grounded in the worldviews and values that we hold.
![]() The Health
Onion is:
The Health
Onion is:
1. Wholistic,
2. Concerned with all health determinants ( not just treatment),
3. Based on individuals at the core then layers of community, living and working,
socio-economic, cultural and physical environmental determinants,
4. Places each layer in context of its neighbours (with structural constraints),
5. interdisciplinary,
6.makes no claim of layers being more important than others,
7. acknowledges the complex nature of health determinants.
Here it is important to consider the global perspectives of Natural and Human science as drivers behind the practices that psychologists follow in their research or knowledge production of health experiences.
Table 1.5 presents important
features of these views.
![]()
Other methods used (See Marks et al (2015):(Participatory) Action Research; Diaries, Blogs and Narratives; Discourse Analysis, Ethnographic Methods; Focus Groups, Grounded Research; Historical Analysis; Intrepretive-Phenomenological Analysis; Interviews; Power Analysis...
Early
History
Psychosomatic Medicine begins with Studies in Hysteria
(1895) by Sigmund Freud and Joseph Breuer who outlined the relationship between
the mind and body, showing that the mind can cause physiological symptoms.
Mind-Body Problem revisited
-Cartesian Dualism
- Mind affects body & body affects minds
Health
Psychology
had
a more formal beginning as early as 1911 when APA
had a symposium on "The Relations of Psychology and Medical Education"
First
world war found psychologists working in applied areas where people like Ned
Bott (1887-1974)
at
the University of Toronto began studies and practice in the rehabilitation of
soldiers returning from war. Not
only did he develop machines to carryout physical therapy (mechanotherapy)
but he also recognized the mind and the active role of the individual in his or
her rehabilitation.
Also
in the early part of the 20th
century physiological studies examined
aspects of human biology that later became standard studies in biological
psychology, such as those by Walter Cannon (1935) on stress and strain in the
autonomic nervous system.
World Health Organisation (WHO) recognized the physical, mental
and social components to being healthy and enjoying a good quality of life in
the 1940s post war time.
Wolff (1950) brought to bear the relationship between
stress
and adaptation in health and disease states
Hans Selye (1956),
The Stress of Life,
interest grew on the
relationship
between thoughts and physiology (akin to placebo
effects).
Schwartz & Weiss (1977)
Behavioural
Medicine is born out of psychosomatic medicine
Behavioural
Medicine
emerged later (1977) as a broad and interdisciplinary field of study that
involves: scientific investigation, clinical practice, and education that
addresses health, illness, and related physiological functions.
Topics
include: Stress & Coping, Coronary Heart Disease, Hypertension, Pain,
Smoking, Food abuse/disorders, Ulcers, Migraines, Asthma, Diabetes, Compliance
with Medical Intervention, Patient & Care Provider Behaviours.
Development
of Health Psychology as a Discipline
According
to your text the development of health psychology as a discipline begins
with behavioural medicine and the Yale Conference of 1977.
1983
–Neal Miller’s article outlines behavioural medicine as the synthesis of
laboratory research and applied clinical work.
He
outlines the biomedical model that is based
upon germ theory, suggesting that disease
arises through infecting of bacteria or other micro-organisms.
Miller
came from a behaviourist background
but also was involved in bridging it with psychoanalysis. His work came to focus
on the relationship between behaviour, personality and health reframing other
concepts in terms of behavioural reinforcement.
Expansion to include cognition and
personality
Krantz
in the 1980s also came to review the field but brought more attention to mental
(cognitive) and idiosyncratic (personality) factors than did Miller’s review.
Type A personality came to garner a great deal of attention
and methods of cognitively restructuring
one’s situation came to be more prominent as a form of therapy, as part of the
larger ‘cognitive revolution’ in psychology.
More attention on coping and
responses to stress came to the forefront during the 1980s as well, as Health
Psychology was taking a larger profile in the field. Thus coping
styles such as blunters and monitors were emerging as psychology was
turning toward more individual attributions of disease.
Psychoneuroimmuniology (PNI) – Is another area of health psychology that has emerged since the 1980s. With a greater emphasis on the immunological aspects of HIV/AIDs and Cancer, more and more attention was paid to the relationship between the mind and the immune system.
Technological
advances in the study of immunocompetence
also made possible the detailed analysis of psychological states and immune
responses.
Why
has Health Psychology come into Prominence?
Changing profiles of health and
illness in Canada
As
in the united states, health and illness profiles have changed over the past
century. What were once regular concerns are no longer of great concern while
other diseases are of greater concern to our aging population. (See
figure 1-1) ![]()
Lifestyles
have also changed with mechanization and more ‘whitecollar work’ while
activity and diet have come into focus as well ( see figure 1-2)![]()
Canadians
have indicated that Health Care (and education) are of highest importance.
Psychologists too are turning more and more towards issues of health as part o
their research and practice.
Marks et al also discuss
global trends in mortality statistics.
![]()
![]()
Furthermore they also
present a refinement of epidemiological statistics in the form of
Disability Adjusted Life Years (DALY) "the sum of
years of life lost from premature mortality plus years of life with disablement
adjusted for severity of disablement from all causes, both physical and mental."
(p. 13)
![]()
![]()
Multiple perspectives are needed
Poole et al (2008) identify the role that studying health psychology plays in understanding statistics about medical issues, including reports from <health Canada> For example when considering reports about cancer biomedical researchers will focus on one aspect of the disease, while psychologists will likely focus on another.
Economists, sociologists and medical geographers will
focus on other aspects of health and illness as well as medical anthropologists
and epidemiologists.
As
they also report, Engel (1997) introduced the biopsychosocial approach.
Marks et al report that this bio-psycho-social approach tends to be a refined
version of the natural science "medical model"
Health
Psychology Today
A bio-psycho-social approach
Has taken a forward role in the field in contemporary health psychology. While it to the forefront in the 1980s it has a long standing tradition elsewhere in psychology and philosophy of science.
This is seen in the works of Erik Erikson,
John Dewey, Wilhelm Wundt and Karl Popper among others.
The
BPS approach implies that clear communication among social science researchers
and health care providers is crucial to understand the big picture of health and
illness.
Medical
practitioners typically are grounded in the perspective of the biomedical
model while other researchers may be more concerned with social
relations, interactions and the role of the mind and subjective
experiences.
Prominent theories in health psychology
1)
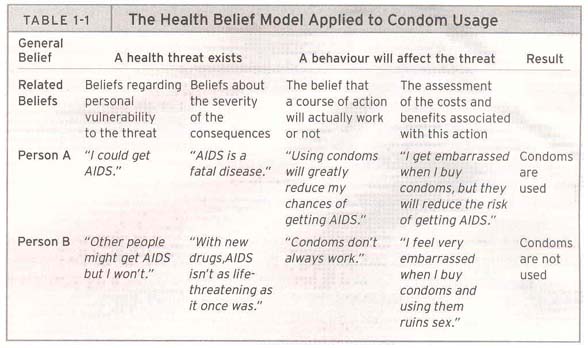
Health Belief Model (HBM)–
stipulates that we have ideas that we believe to be true that have an impact on
our health (Becker, 1974; Rosenstock, 1974 cited in Poole et al, 2005).
In particular beliefs about behaviours and their impact on health are of
interest.
Health belief systems, or clusters of ideas are also of interest insofar as they may be related such as inevitability, impact of consequences, and ability to control.
Examples gives include: efficacy belief
or one’s estimate of the workability of a course of action or treatment as
well as cost-gain belief that pertains to
one’s evaluation of the outcome of an action.
<See table 1-1>
![]() for beliefs
regarding HIV/AIDS
for beliefs
regarding HIV/AIDS
An individual may harbour contradictory
beliefs which may or may not be resolved by cognitive dissonance.
Values
also
play a role here where one may hold a health belief but place little or no value
in good health.
There may also be
economic, gender and political differences
in the affordability of holding or valuing specific health beliefs.
The health belief model has had variable
success in predicting health behaviour. Some studies reported by Poole et
al report some success while others have had little.
![]()
2) Theory of Reasoned Action (TRA) – is similar to the belief model but it assumes that prior to action is intention (Fishbein & Ajzen, 1975).
It involves both attitudes about specific behaviours as well as one’s beliefs about others’ perceptions and expectations as they play a role in our development of subjective norms.
Based
upon our own understanding of our attitudes and subjective norms we develop
intentions for action.
<see Table 1-3>![]() for examples of two
possible outcomes.
for examples of two
possible outcomes.
According to Poole et al., The Theory or Reasoned Action does a good job to predict HIV risk avoiding behaviour and cancer screening behaviour.
3) Theory of Planned Behaviour (TPB)- is an extension and 'update' on the TRA. It is expected to provide increased predictive power based upon perceived behavioural control[over and above intentions or beliefs] (Fishbein & Azjen, 1975).
Locus of Control
is central to this theory which pertains to one’s perception of one’s
ability to control one’s fate or the outcome of a disease or condition.
Various measures have been developed such as the Multidimensional Health Locus of Control Scale (MHLC) for assessment and prediction of behaviour. This provides scores on three scales: internal, external and “powerful other.”
Institutionalization
often leads to loss of control and lesser health outcomes.
Learned helplessness is a condition resulting from severe loss of control and has been associated with depression and poor health.
Gurung (2006) discusses the cultural aspects of planned behaviour, indicating that it applies differently in different cultures, e.g. increased peer influence on adolescent smoking among Whites & Latinos vs. African Americans in contrast to the increased parental influence on alcohol use among African Americans vs. than whites.
Here the subjective norms (cultural values) may add predictive value to the TPB.
4)
The stages of Change model : The Trans-theoretical Model – describes the ways in which carryout change
through six stages (Prochaska & DiClemente, 1983). Eg, smoking cessation. ![]()
1) precontemplation, 2) contemplation, 3)
preparation 4) action, 5) maintenance, 6) termination, (7? relapse).
Working
in Health Psychology
Clinical and counseling psychologists
Research Careers in health
psychology
International Health Psychology
Aboud (1998) has extended the general model of health psychology to an international perspective which covers such topics as:
Genetic and biological factors (sickle cell anemia, age, gender)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}