Pain
Overview
The Significance of Pain
Pain Perception
Theories of Pain
Gate control theory
Neuromatrix theory
Neurochemical Basis of Pain and Pain Inhibition
Acute versus Chronic Pain
Psychosocial Factors and Pain
Gender differences
Cultural differences
The Measurement of Pain
Psychophysiologcial measures
Behavioural assessment
Self-reports of pain
Assessing Pain in infants and children
Assessing Pain in older adults
Pain Control Techniques
Pharmacological control of pain
Surgical control of pain
Transcutaneous electrical nerve stimulation
Accupuncture
Physical Therapy
Massage
Relaxation
Distraction
Biofeedback
Hypnosis
Multidisciplinary pain management programmes
The Significance of Pain
Pain has an evolutionary value, it keeps us avoiding danger and 1) stops us before serious injury happens, 2) prevent further injury, through learning, and 3) provides a brake on activity to ensure healing and recovery.
Pain Perception
Various theories of pain are present, each building from the basic physiology of pain.
Afferent sensory nerves carry signals from
nociceptors, pain receptors.
Two types of fibers are present, A-delta- fibres ( small, myelinated, fast) and C-fibres (large slow, non-mylenated). The relative balance of activation of these fibres gives rise to pain or not.
Theories o f Pain
Gate Control Theory of Pain Signals passing through the spinal chord "gate" to brain lead to experience of pain. Some neurons open and some close the (inhibitory) gate.
| Three Components to the Gate A-delta fibres |
Two fibres and one
interneuron C-fibres | |
| Slow- small | Inhibitory | Fast large fibre pressure |
| dull or chronic pain |
Inter- Neuron |
"emergency" signals |
-also have descending cortical nerves to close gate
-slow (small) fibers inhibit the inhibitory inter-neuron and activate the projection (pain) neuron, opening the gate and giving PAIN
Phantom Pain - aching, burning or sharp pain in a limb or organ that had been amputated. Why? See video from you tube of VS Ramachandran @ 3:30 (prt2)
Two possibilities:
1) Impulses that had previously
closed the gate are reduced or lost
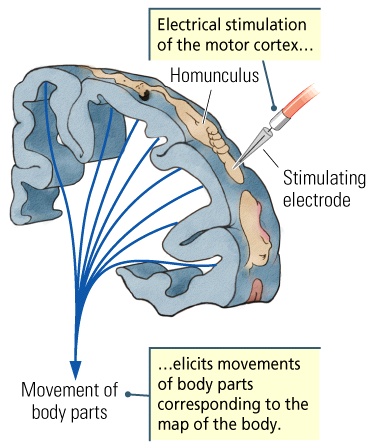
2) Once pain producing activity begins in the
brain it continues without sensory input (being stimulated by neighbouring brain
areas-i.e., face-hand)
![]()
![]()
3) Other brain parts are "calling" the missing limb.
Anomalies: People born with missing limbs have never had
normal sensory experiences why do they experience phantom fingers or
toes?
Neurochemical Basis of Pain and Pain Inhibition- midbrain area - periaqueductal gray electrical stimulation leads to a blocking of pain. This is an example of a stimulation-producted analgesia.
Endogeous opioids - natural brain chemicals that regulate pain. Found in the brain, spinal chord and glands, they act on brain sites that are also acted upon by heroin, opium & morphine.
Acute versus Chronic Pain acute-short term, chronic-ongoing are seen in various forms such as chronic recurring, chronic intractable benign, responded, operant pain and pain behaviours.
Psychosocial Factors and Pain
Gender differences - some suggestions that women have lower pain threshold and levels of pain tolerance. Others studies refute these claims suggesting that men tend to report less pain due to social expectations.
Cultural differences - meaning of events and expectations of pain vary.
The Measurement of Pain - difficult to measure, almost no overt behaviour for it.
Psychophysiologcial measures : EMG, autonomic activity, electronencephalography, evoked potentials.
Behavioural assessment : non-verbal facial and vocal cues, postural form, movement, supplemental spousal diaries and estimates of pain.
Self-reports of pain : interviews, rating scales (visual analog
scale, box scale, verbal rating scale) <see Figure 10-1>
![]() . Pain questionnaires also are useful, such
as the McGill Pain Questionnaire (MPQ)
. Pain questionnaires also are useful, such
as the McGill Pain Questionnaire (MPQ)![]() or the West
Haven-Yale Multidimensional Pain Inventory (MPI).
or the West
Haven-Yale Multidimensional Pain Inventory (MPI).
Assessing Pain in infants and children - is often very difficult
Assessing Pain in older adults - also has limitations
Pain Control Techniques
Pharmacological control of pain
Peripherally acting analgesics
- non-narcotic
analgesics act on entire body (ASA, Ibuprofin).
Centrally acting analgesics - narcotics opium, morphine, codeine as well as Percodan & Demerol.
Local anesthetics - acting topically or through injection, i.e., novocaine.
sedatives & tranquilizers - not really blocking pain, but relaxing and enhancing the effect of others through additive effects.
Surgical control of pain - severing the nerves to spinal chord or to brain. Not always working well, (see phantom pain).
Transcutaneous electrical nerve stimulation - electrodes placed on skin
(non-invasive).
![]()
Acupuncture -
balance and flow of qi
through the
body, to ameliorate the pain.
![]()
Physical Therapy
Massage - various types (Swedish, Shiatsu, Tai Chi.
Relaxation - progressive muscle relaxation, guided imagery <the Matrix>
Distraction - changing focus of attention and reinterpreting what is there.
Biofeedback - electrico-mechanical information feedback about the state of the body.
Hypnosis - effective in cutting reports and over behaviour of pain (cold presser) but also showing subtle signs of pain, through ANS as well as hidden observer.
Virtual Reality
![]()
Multidisciplinary pain management programmes - bringing together the talents of professionals from a host of areas to provide a broad and comprehensive program. Such points of concern are: perception of pain, improving physical lifestyle, social support, reliance upon medication, use of healthcare facilities.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}