Table 11-2
Health Psychology of Cancer
Negative
& PositiveMood and Cancer
Poole et al report that depression, a sense of hopelessness, or persistent pessimism increase the risk of getting cancer and decrease one’s chance of surviving it.
Schmale & Engel (1967) found that patients who were “giving up” or had “given up” in their fight against cancer.
Sheklle et al. (1981) provided stronger support for this link between mood and cancer through a longitudinal study of healthy individuals. After 17 years it was found that those who scored as having clinical depression (by the MMPI) were 2.3 times more likely to die of cancer than those who didn’t.
Likewise Schultz et al. (1996) have shown that pessimism is related to decreased survival rates among 30 to 59 year olds.
Poole et al also point out that not only does immunocompetence explain these results, but also behavioural changes due to diagnosis of cancer and /or depression (e.g., following regimens, self-care, sleep, smoking, …) will have an impact on health.
Positive Mood and Cancer
Holland & Holahan (2003) demonstrated the benefits of social support, while Levy et al. (1990) have shown that women with cancer who have emotional support have higher NK cell levels.
Others have shown that social support is associated with longer survival while those who are socially isolated are twice as likely of contracting hormone-related cancer.
Cancer A serious illness whose mortality rates peaked in 1989 and have since dropped to rates similar to the 1970s, but is growing in incidence. <Stats Can> Probability of developing cancer over lifetime is 35-40% and increases with age.
It is actually several
diseases that are related in general but vary across specific sites and forms.
Oncologists specialize in
site types of cancer, each diagnosing and treating.
When cancer spreads from one area of the body to become a more general disease it is metastasized.
Physical problems - fatigue and Pain are most commonly reported complaints.
Pain management is a challenging affair where many patients are afraid of over taking opiate-based medication, while other forms (SSRIs) may be harmful.
Psychological distress - fear and depression are biggest factors.
Fear is often found with respect to body integrity (loss), radiation therapy, cancer relapse and death.
Depression is also common, particularly with pancreatic cancer (poor prognosis), and has been related to: poorer quality of life, less compliance, longer hospital stays, higher mortality rates (Newport & Nemeroff, 1998).
Those demonstrating depression also tend to report higher pain levels, and higher caregiver depression.
Intrusive memories may also be a problem where thoughts of cancer or death or other related unwanted ideas or images persist in memory and lead to poor coping.
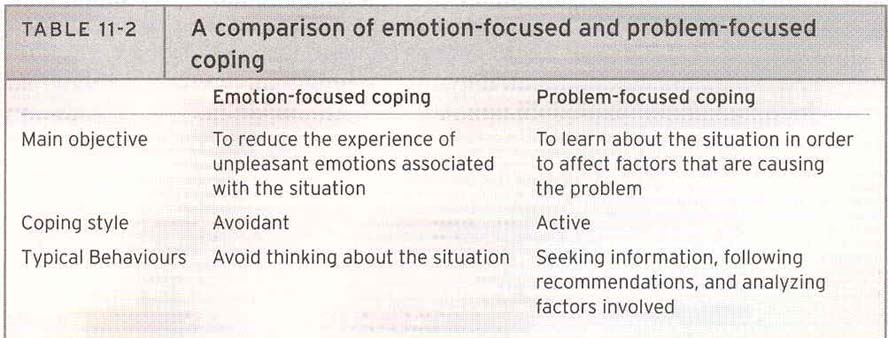
Review Problem vs. Emotion focus & Active vs. Passive coping. Mixed results on
successes.
Table 11-2![]()
Cancer treatment - surgery, radiation treatment, chemo therapy. <Image>![]()
Once again fear is a big factor here, fear of the treatment, not the disease.
Radiation therapy - radiating the location of tumor as outpatient with mask, mould, or mark (tattoo) to maintain the exact location for treatment.
Chemo Therapy - strong drugs that kill cell growth, produces powerful side effects: fatigue, nausea, hair loss, loss of mucous that can be painful and cause diarrhea.
Anticipatory nausea occurs through classical conditioning of the bodily response to the cues associated with chemo dosages (food, place, clothes, smells).
Helping people cope with cancer - social support is important here, as elsewhere, where family orientation (coping abilities) can have an additive impact on the patient.
Communication styles and goals are presented by Poole et al. where they indicate that the helpers must support the concerns and fears as legitimate while also attempting to help alter or adjust perceptions for coping.
Navigators are also used to help with help make it through the process, while community group or patient support groups can help with information and empathic support.
Monitors and blunters will vary, however, comparisons in and upward or downward direction are likely to occur to acquire hope and reduce despair.
Psychotrophic medication and therapy may be used, but such medication may lead to complications. Group and individual therapy is beneficial for many.
Personality & Cancer
Eysenck et al. (1989) have suggest that type 1 personality, those who feel great loss when prevented from being with a valued object or person, tend to experience elevated stress levels and are more prone to cancer than other types.
Also known as Type C personality, some people are"pleasers" who draw self sesteen from how others see them and keep their feelings (i.e. anger, fear, sadness) hidden "keeping "face".
Marks et al. (2015) identify "distress proneness" as a tendency for people to engage in pessimistic explanatory style, and to be low on: self esteem, self-efficacy, hardiness & coherence.
TCM & Cancer (Zhu
Chapter 13) - The best of Both Worlds
- Herbs to accompany traditional
western cancer therapies. Patients who receive treatment from both Western and
TCM practitioners will receive treatment for the local site of the cancer as
well as the whole body.
-
Here the intent is to eliminate the pathogen as well as replace vital energy of the body.
Herbs that attack cancer cells and others that remediate the condition of the body are given along with foods that have been shown to heal or help to fight cancer.
Prevention is also important where a balanced diet of specific cancer fighting foods can increase health and longevity.
Some such foods include: soybean, bok choy, celery, cabbage, lo bok, carrots, hot peppers, tomatoes, cucumbers, eggplant, pumpkin, bitter melon, broccoli, green peas, sprouts, and green tea.
For terminally ill cancer patients acupuncture can be used for the pain and herbs to reduce water and energy.
{kind=link}
{kind=link}