Communication
in Medical Settings
& Adherence to Regimes
Overview
Perceiving and
interpreting symptoms
Seeking medical care
Delaying medical care
Physician-Patient
Interaction
Basic Models of Physician
Patient Care
Physician-Patient
Communication
Intercultural
Communication
Adhering to Medical
Advise
Assessing Adherence
Frequency and Cost of
Non-Adherence
What factors Predict
Adherence?
Improving patient Adherence
Health Outcomes
Communication in Medical Settings
Issues of communication abound in Health Care and in Psychology
They begin with being able to understand and articulate one's condition and end in receiving or maintaining optimal health. All too often challenges of communication limit the Health Care one can receive, leading to ill health and disease as well as tragedy and even death.
Perceiving
and interpreting symptoms
Prior to reporting symptoms one must first notice or perceive them as such. While one may see or feel something for it to be understood as a symptom of a disease or condition it must be perceived as a symptom worth taking note of.
Individual differences exist in terms of attention paid to ones own body or condition, self-monitoring is a psychological trait that involves paying a good deal of attention to ones own states or statuses.
Accuracy is also important that once noticed one recognizes a real symptom as being present and not have a false alarm or miss. Those who believe they are likely to contract a disease are more likely to notice symptoms, whether real or imagined (i.e., Woody Allan).
Stress also may play a role here where symptoms are exacerbated or initiated. Changes in physiological states due to stress may be mis-perceived as symptoms of some other disease or illness.
Ones
state of mind or mood also plays a role where those
who are in good spirits tend to perceive their health as better than those who
are in negative moods.
External stimulation or engagement in activities (mental and physical) tend to distract people from symptoms, unless reminded by those sources.
Cognitive abilities and attentional capacities may also play a role.
Age also has been shown to play a role in noticing symptoms where older persons tend to be less vigilant of symptoms than younger people in noticing cancer symptoms.
If
considered commonplace may be disregarded while some cultural expectations in
terms of health and coping (stoicism) will differ (e.g., reporting vision
problems Canada vs. US).
Seeking
medical care
Once noticed and interpreted as something to pay attention to, people may or may not actually seek medical advice or care.
Poole et al report that we make use of a lay referral system, influences of others around us who tells us that we look healthy or ill, need to see a doctor or not to worry.
They also report that while 75 to 90 % of people might perceived relevant symptoms, only about 30% actually seek assistance. This rate may be different for various body parts or ailments.
Lyons & Chamberlain
(2006) discuss the Health Belief Model regarding seeking medical help.
![]()
Delaying
medical care
Ambiguity over the nature of symptoms is likely to delay seeking treatment, especially for cardiac arrest which may be interpreted as gas, indigestion, ulcer, flu, or muscle (arm) pain. Generally symptoms emerge two to fours hours prior to myocardial infarction, this leaves a good deal of time to interpret and react.
Embarrassment may also play a role in delaying help seeking, once symptoms have been noticed, where one may not want to talk about the symptoms (i.e., Guy LaFleur & Male ED).
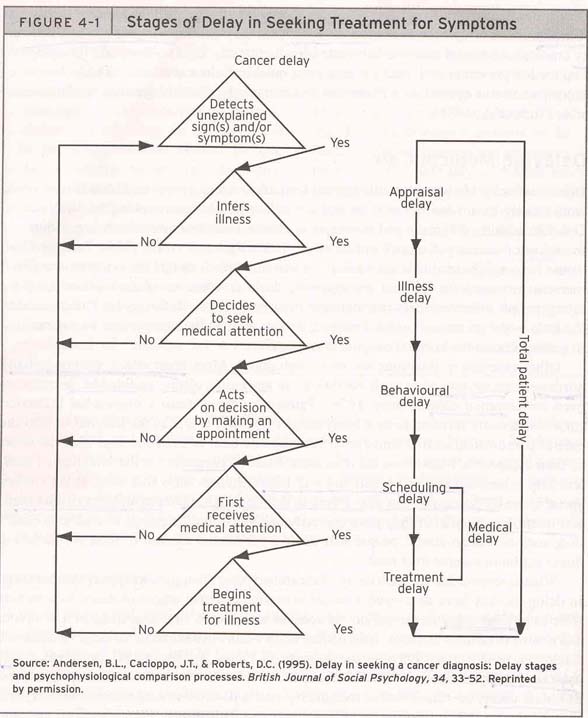
Anderson et al. (1995) suggest a four-stage process for patient delay - time between first notice of symptom and treatment of those symptoms.
1) appraisal
delay time taken to notice and interpret symptom as sign of illness
2) illness delay time taken from realization of
illness to decide to seek treatment
3) behavioural delay time taken from decision
to actually seeking treatment
4) medical delay time taken between first
making appointment to actually receiving medical care.
<see figure
4-1>![]()
Generally those who experience the least amount of pain
are slowest to seek treatment,
while those in greatest pain demonstrate the
least delay.
Additionally those who experience new or changing symptoms are also more likely to seek treatment vs. those who have had the same symptoms for some time, along with those who imagined themselves as being severely ill.
Fear
also plays a role here where high fear and low fear may prohibit people
from seeking medical attention, while moderate levels may be most motivating to
seek treatment. Fear may involve
death, disability, financial, social or marital loss.
Societal
or role obligations and keeping busy with others or living day to day may
also play a role in delaying the seeking of treatment (e.g., middle-age
parents).
Age
may play a role but studies are not consistent, although Ramirez et al. (1999)
report that older women may have longer patient delay while younger women may
experience longer medical delay in seeking treatment for cancer.
Gender - Lyons &
Chamberlain (2006) indicate why women tend to seek medical care more often
than men.
![]()
Physician-Patient
Interaction
Patient vs. client what language is best?
Traditionally in the medical model the term patient has been used which connotes a sufferer, a passive recipient of treatment, one that is acted upon.
The term client connotes a more active role of someone who is under the protection or guidance of a professional.
According to Poole et al, most people prefer the term patient, indicating that the term client may lead to a denial of the illness or blaming the client for his/her condition.
Basic
Models of Physician Patient Care
Szasz & Hollender (1956) outline three basic models of physician-patient relationship;
1) Active-Passive model considers the patient as a passive recipient and unable to participate in his or her own care.
2) Guidance-Cooperation model indicates that the patient seeks advice, answering questions and relying upon the physician to determine the diagnosis and treatment.
3)
Mutual-Participation
model assumes that the physician and patient share the
responsibility of decision making about diagnostic tests and treatment(s).
Power is an important issue here where the first model places all of the power with the physician and the last one demonstrates a sharing of power between the physician and patient.
Roter et al. (1997) offer a different model, based upon audio-taped conversations, or communication styles, between physicians and patients.
1) narrowly biomedical focused on closed-ended questions (i.e., does it hurt when ?)-32% of visits showed this.
2) Expanded biomedical still closed-ended questioning but allows for more psychosocial exchange (i.e., how do you feel? ) (33% of visits)
3) Biopsychosocial style - shows a greater balance of the biomedical and psychosocial styles (20%)
4) Psychosocial - greater focus on psychosocial exchanges and advice (8%)
5)
Consumerist - approach focuses on the
questions of the doctor by the patient, seeking to acquire information from the
physician (8%)
Poole et al suggest that patients prefer the psychosocial or collaborative model while physicians preferred the consumerist style.
Lyons & Chamberlain
(2006) discuss patient satisfaction & confidence
![]()
Question: which do you prefer? Why? See activity 4
Physician-Patient
Communication
Various aspects for the communication process are important to consider: information, participation, patient satisfaction, malpractice claims, barriers to effective communication.
Information Giving - is a primary role of the physician, however this does not always occur with respect to diagnosis, causes, or treatments. Patients may want to know more information and Physicians may think they are giving more information than they actually are.
Limited information giving may be due to apprehension in creating anxiety or trying to protect the patient, or through thinking the patient will not comprehend the information.
Participation - pertains to the desire for patients to play an active role in their healthcare. While this is the stance desired by many younger patients, many older patients may prefer less participation.
Physicians may also vary in their desire and degree of openness to participation not only with patients but also with other colleagues.
General patient satisfaction - is largely determined by the pace and style of the physicians communication. Personal factors like warmth, emotional expression, friendly, confident are more likely to lead to satisfaction.
Malpractice claims - are more likely to occur when the patient is dissatisfied with the physician, including their communication style.
Poole
et al indicate that understanding the patients expectations
and perspectives is crucial to avoid litigation and malpractice.
Barriers to
communication
Physician behaviours - interrupting the patients and not eliciting their concerns or perceptions. Studies have shown that interruptions may inhibit the central concern from being reported as well as actually take longer to complete the visit.
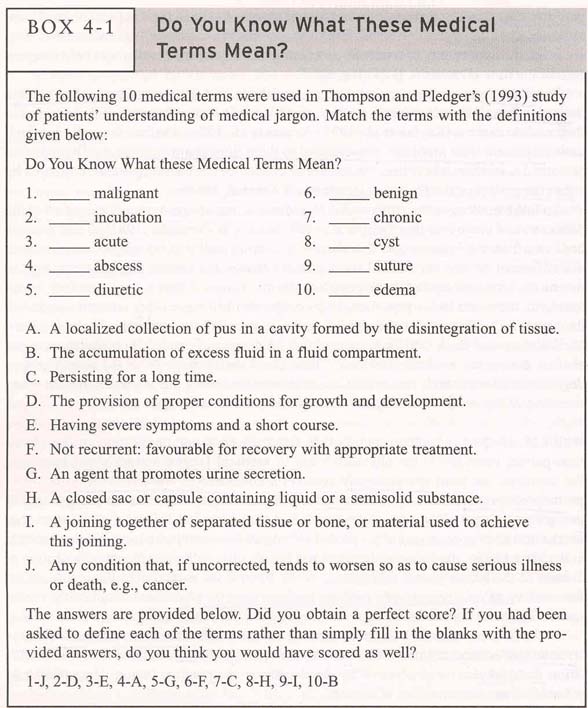
Medical
jargon also may leads to misunderstanding and poor communication,
where physicians may assume that patients understand them or they may not
actually want patients to understanding them (mystery-mastery complex).
<see box 4-1>![]()
Poole et al suggest that the best place between jargon and baby talk is to make use of:
Non-discrepant responses making use of the same vocabulary as being asked by the patient, as well as,
Multilevel explanations making use of medical jargon and then clarification in lay language.
Time factors are also important where the visit and communication may be altered by the pace and time available for the consultation.
Patient-centred or doctor centred encounters may occur, where the psychosocial or biomedical style may be found. Poole et al report that negative visits may actually take longer than positive visits.
Patient volume also plays a big role in time available and patient satisfaction, where big volume physicians tend to give lowered patient satisfaction.
Patient behaviours deception may be present where patients may hide or fail to reveal aspects about their health or behaviour.
Failing
to ask for information may also occur because of:
1) doubt or thinking it was not up to them to ask
2) afraid of what the doctor might think of them
3) afraid of a negative
reaction from the doctor
4) too flustered or
hurried to ask
5) doubted the doctor could tell
them more
6) forgot to ask
7) feared the truth
Memory may cause problems where people tend to remember the gist of things, and reconstruct events of the past.
Anxiety also can make it difficult for patients to remember or concentrate on the diagnosis or treatment.
Lyons & Chamberlain
(2006) - The Active Patient
![]()
Intercultural
Communication
Culture plays a number of important roles in communication in health care. Part of its effects are due to the nature of culture and relationships, others have to do with specific aspects of communication, i.e., verbal & non-verbal. Samovar & Porter (2004) outline a number of areas where inter-cultural communication play a role in Health Care.
Family roles play an important role in the manner in which health care is sought and received
1. Male dominance - may lead to the situation where only the male (head of the household) is to be spoken to. Alternatively the mother may not answer questions to a male doctor or in the presence of her husband. It might be best to ask both the wife and the husband in order not to offend either of them.
2. Modesty and female purity - For many cultures women should be treated by female doctors and nurses and males by male doctors and nurses. Illness may affect the honour or purity of women and their prospects for marriage. Thus secrecy about illness is often found in some cultures where disclosure to medical staff and to friends and community members is found.
3. Pregnancy and childbirth - surrounded by cultural values and practices. Expectations for women to bear children are present and when that should occur. Contraception is often seen taboo in cultures. Who is present at the birth varies from culture to culture as does the expression of pain, sometime eliciting gifts (Iran).
Self-disclosure - Cultural norms vary about the type and amount of information to be disclosed. Clearly in a health setting this can be serious and form a significant barrier to suitable healthcare. Example in the text indicates that in translation it might appear that adequate consent is being achieved, but the barriers for sons and mothers or fathers and daughters to talk about certain issues my not offer accurate information.
Language barriers - Challenges of translation occur where literal
translation may not be possible. Where medical treatments require accurate
information the consequences of false info can be detrimental and serious.
The patient may hard time telling what is ailing them due to a dearth of
language.
Accents may also cause some trouble where clear communication is
difficult.
Nonverbal messages
1. Eye contact - as in other areas of communication different standards in eye contact may lead to interpretations of disrespect or hostility for one of the individuals. This may damage the relationship between health care provider and patient.
2. Facial expressions - may lead to miss communication such as smiling that might indicate politeness or happiness. The medical professional might misinterpret it thinking all is well (e.g., counselling).
3. Touch - also have varied standards for how and where medical professionals can touch patients. This may lead to serious situations for certain issues, especially when gender is involved. Elsewhere touch can be seen as a method for cure, or causing disease-laying on of hands or touching the head.
4. Time - is important for when one is to show up for an appointment, how long to wait and the impact on mood of mental state as a result of conflicts in time expectations.
a. Informal time (tardiness and pace) - expectations for when to arrive and what it means to be late: NA 5 minutes vs. Indian 1 hour or 2 hours for Italian and maybe not at all for Javanese.
Pace is how fast things happen and how fast to expect service or action.
b. Past, present and future orientations
- Past-oriented cultures have a strong sense of tradition and custom.
-Present oriented cultures tend to enjoying and living in the moment
-Future oriented cultures tend to emphasize planning ahead- low tolerance for postponements but more interest in change.c. Monochronic (M-time) and polychronic (p-time) classifications
M-time is characteristic of "western" cultures that view time as a fixed linear process to be scheduled and rationed.
P-time is characteristic of "collectivist" cultures that have amore holistic view of time where they can interact with many people at once and carryon various activities with interruptions.
5. Silence (cross-cultural and co-cultural differences)
This can be difficult to managed in an intercultural setting where expectations of having to fill the silence may be at odds with expectations of having the silence.
Formality of language use and addressing others as well as greeting behaviours.
Notions of politeness, Chinese three refusals, agree to follow prescribed action but not understand what it is or even wish to follow it.
Adhering
to Medical Advise
Compliance is a term used to describe adherence to medical regimen, however it connotes obedience.
Adherence may involve taking medication, changing life style, eating habits, exercise, or abstinence.
Non-adherence may be outright or may be creative non-adherence in one form or another where a variation on the treatment might be found (i.e., taking double dosages).
Assessing
Adherence
Various subjective methods may be used here ranging from asking the health-care provider to the patient him/her self, to family or friends. Challenge of accuracy & honesty remain.
It may also involve objective measures such as counting pills, biochemical evidence or treatment non-response. Challenges of measurement still arise, (i.e., discard, cost, )
Frequency
and Cost of Non-Adherence
Estimates of non-compliance are around 50%, but could range from 0 to 100. DiMatteo (1994) suggests that there may be 43% non-adherence to long term treatments and as much as 75% non-adherence to lifestyle recommendations.
Economic Cost to Canadians in billions of dollars? Due to productivity (sick days), ambulatory costs, acute and extended care costs, and premature deaths.
Personal costs of
reduced health and quality of life are significant.
What factors Predict Adherence?
Type of treatment
regimen duration & complexity- may have an impact on adherence, such as
long-term behavioural changes, which may take a considerable time and effort
and may require a complex treatment of
integrated techniques.
Severity
of illness at very low and very high levels may lead to non-adherence
through dismissal and giving up. Severity
of pain appears to be correlated with adherence.
Age
Thomas et al., 1995 report 70 year olds best and over 80 as well as
under 50 were worst at adherence. Cognitive deterioration and busy life style
are attributed to these groups.
Gender
women may be better than
men at adherence to dietary restrictions and taking medication for mental
disorders, however no difference reported for antihypertensive,
diabetic, or exercise maintenance were observed.
Cultural
or Ethnic Differences have
not been widely observed but there is a possibility of following alternate
healing or health approaches that may consider adherence or other regimens un
important.
As
above, physician characteristics are also important where his or her style of
communication, relationship and personality all may play roles in adherence of
patients.
Their interactions, expectations and communication all must be supportive of adherence, otherwise it may not be likely.
Improving patient Adherence
Poole et al indicate that social influence of the physician patient relationship will involve social power in one or more types of influence over the patient.
1) Informational influence is expected if the physician can convey the content of communication in a clear and comprehensible fashion.
2) Reward power may also be present where the health care practitioner provides the patient with tangible and obtainable rewards
3) Coercive power involves manipulation and possible punishment for non-adherence, i.e., attempts to withhold service.
4) Expert power is invoked when one makes a plea for adherence based upon the expertise or knowledge authority of the healthcare provider.
5) Legitimate power is used when the patient accepts the demands of the provider without the need for coercive power.
6) Referent power is when the patient identifies with another who serves as a reference or model of adherence.
Reactance may occur where the patient regains a sense of control after having relinquished previously and stop compliance with a treatment regimen.
Internalisation is most important for long term adherence where beliefs and behaviour might be
expected to change. Self-motivation and education may playa role here along with
cohort effects in terms of getting information and making it part of ones
identity.
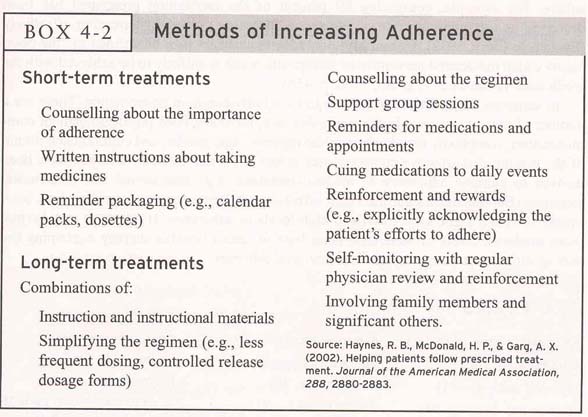
Behavioural
strategies are also effective, making use of prompts and reminders, along
with suitable rewards and reinforcers. Self
awareness or monitoring is often encouraged,
Social
Support again is potentially very helpful where encouragement and
emotional comfort along with informational and practical support can be
effective.![]()
Health Outcomes
Appear to be more positive with greater adherence to medical regimen and treatment.
Improving
multicultural health care interaction
-
medical culture is often not understood, even by people from the same general
culture
Recognize that a culture may rely on several medical systems - Currently in Canada and the US there are a wide variety of medical practices that range from mainstream to marginal. In psychotherapy and counselling as well there are a wide variety of orientations that may be used.
Must acknowledge patient's beliefs concerning the causes of illness, how illness should be treated, and how it can be prevented. Perhaps there needs to be a mixing or blending of traditions use to achieve optimal results, e.g., in text there is example of a Cherokee woman who needed a ceremony before submitting to surgery.
Questions to ask the patient - get to know what their belief system is and what their sense of the source of their problems is. What are their expectations of the healthcare provider and the treatment?
Recognize Ethnocentrism - Standards from one culture or sub-culture that are used to judge others represent ethno-centrism. This include notions of health and wellness, disease and cure. Sensitivity to these issues is important for all involved, particularly professionals in the healthcare industry.
Gary Geddes has also recently chronical Medicine unbundled: A journey through the minefields of Indigenous healthcare.
Additional sources:
Samovar & Porter (2003). Intercultural communication. Belmont CA: Thompson Wadsworth
{kind=link}
{kind=link}
{kind=link}
{kind=link}