Clinical Cultural Psychology
Psychological syndromes and Disorders across cultural worlds
Each perspective in psychology provides a unique view on psychological conditions, syndromes and disorders.
The specific emic perspective that is considered provides an account of what is normal and expected, including those epi-normal and abnormal conditions that are considered to require treatment or therapy.
Cross-cultural psychology looks at psychological conditions from two perspectives: universality and cultural specificity.
Those who move towards the ideal of a universal psychology look for cultural conditions and syndromes as being consistently present across all cultural possibilities (i.e. DSM).
The second view considers cultural variation on the presence and form of cultural conditions to be varied across observed cultures. There is usually an assumption that there exists a universal basis to the disorders that is altered in expression within a cultural context.
The more extreme view is one that more closely resembles a cultural psychology perspective where the assumption of an underlying universal basis to psychological conditions is abandoned.
Berry et al. (1992) discuss various
psychological syndromes
and "disorders" as they occur across cultures: Box 15-2;
![]()
Matsumoto & Juang (2004) describe research on abnormal behaviours across cultures
Schizophrenia - Characterised by a collection of traits: distorted sense of reality, withdrawal from social interaction, disorganised perception, thoughts and emotions, affected about 1% of Americans. Diasthesis-Stress model that there is a certain underlying bio-medical cause and cultural influence on the course of development and shaping of the expression of the disorder.
WHO study (International Pilot Study of Schizophrenia, 1973 - 1981) reports cross-cultural symptoms as: lack of insight, auditory & verbal hallucinations as well as ideas of reference.
They also report that: course of illness was easier for people from developing nations (Columbia, Nigeria, India) vs. highly industrialised countries (England, US, Soviet Union). Also found US patients to have greater insight and fewer auditory hallucinations than Nigerians.
Critique? Assessment tools - not able to assess culturally unique expressions of disorder. Study looked primarily for commonalities not variations.
Cultural variations in expression and / or diagnosis?
Schizophrenia -
Ireland has four times the admission rates than England. Irish Americans have also been found to have higher rates of paranoid delusions while Japanese tend
to be more withdrawn and passive.
Depression - Characterised as having symptoms of: intense sadness, feelings of worthlessness, and withdrawal from others affecting 3 - 7 % of Americans at any given time by 26% of females and 12% of males across their lifetimes.
WHO study (1983) reports cultural similarities in symptoms for 76% of respondents from Japan, Iran, Switzerland & Canada. Symptoms are: sadness, joylessness, anxiety, tension, lack of energy, loss of interest and concentration.
Marsella suggests that 'vegetative' symptoms are cross-cultural while others find variations in feelings of guilt or unworthiness (Nigerian), somatic complaints (Chinese).
Leff (1977) contends that variations in expression and communication of emotions (ala Sapir-Whorf) leads to differentiation in the manifestation of clinical disorders across cultures.
Mustafaeva (2015) describes metaphors used to discuss depression across cultures:
Chinese - "gloomy/depressed/ frustrated sickness" having "lost meaning, inhibited, constrained, worried and restrained" (p.21).
Japanese - make more use of external referents "dark. rain, cloud"
Korean - colour words like Blue "everything that surrounds me is dark and black"
Punjabi - tend to describe as "weight on heart or mind" gas building up "pressure"and feelings of heat (ayruvedic).
Turkish - also use heaviness metaphor in chest, "squeezed heart"
Taiwanese - use "fan-zao" anxious worried feelings.
Somatization - bodily complaints and conditions that result from psychological distress. Some research has suggested that Hispanics, Japanese, Chinese and Arabs tend to somatize more that do Europeans and Americans.
Other recent
publications suggest that this is not the case,
rather that within doctor patient
conversation there is open expression among Chinese patients and that somatization
is a universal phenomenon.
Mustafaeva (2015) Traditional Chinese medicine locates in emotions in body.
Liver is the source of headaches, epigrastric pain, hypertension & anger (gan zhu nu / nu shang gan )
Heart is source of anxiety, uncertainty & fear
where Emotional distress - unhappiness and worrying are seen to be grounded in heart and liver.
Koreans describe Hwa-Byung as an anger syndrome with depression & restraint, somatic illness (palpitations, headache & heat) and neurotic symptoms.
Dubai - somatic depression is observed in chest having fatigue & lack of body energy (ta' bana) nausea, limb pain & poor appetite (liver-chabid).
Afghan - depression as sadness with guilt - complaints of nervourness & headaches, weakness, tiredness, imbalance and somatization.
Jigar Khun - sadness & grief - following interpersonal loss.
Asabir - nervous - highly stressed - from major life stressors.
Omidian (1996) describes these as:
asabee (asabi) - physical and emotional discomfort
narahat - discomfort &/or anxiety and depression.
Fishar-e-bala - high blood pressure - (agitation)
Fishar-e-payin - low blood pressure (low energy and motivation).
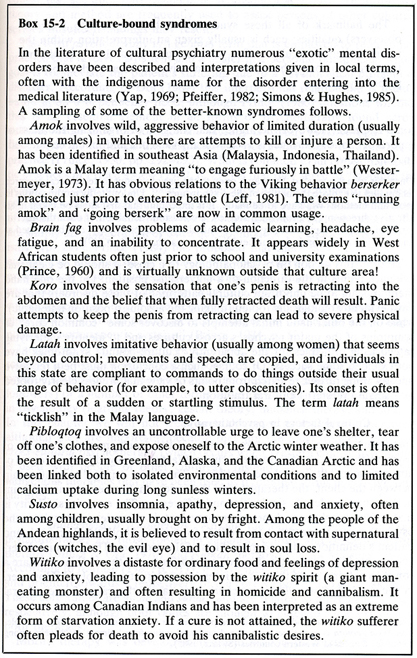
Culture - Bound Syndromes
Berry
et al. (1992) Box 15-2;
![]()
Amok - Found in Asia (Malaysia, Indonesia & Thailand) syndrome of rage and homicidal aggression due to stress, sleep deprivation and alcohol consumption. Is a Malay term meaning "to engage furiously in battle" (Westermyer, 1973 cited in Berry et al., 1992).
Beserker - Viking term of preparedness for battle (Leff, 1981 in Berry et al., 1992).
Witiko - Algonquin syndrome of being possessed by the witiko spirit (man-eating monster) that leads to cannibalistic behavious and suicidal ideations. (due to starvation)
Anorexia Nervosa - distorted body image, fear of becoming fat, serious loss of weight and food restraining or purging.
Found in North America and Europe, becoming more common
in other international urban centres.
Variation in reasons from fear of being
fat to extreme distaste for food to "intollerably full" in China.
Also consider body dismorphic disorder.
Hikokomori - Japanese condition of withdrawal where one rarely leaves one's room and don't interact with family.
Brain Fag - involves suffers of eye strain, concentration and academic studies among west African students.
Ataque de nervios -
trembling, uncontrolable shouting intense crying, heat in chest rising to head
and dizziness.
Found among Latin Americans usually around stressful family
events such as funerals, divorce, witnessing an accident.
Pibloqtoq - the
intense desire to tear off one's clothes and run outside in the deep winter.
Found through the peoples of northern Canada, Alaska and Greenland.
Whakama shame and self-abasement inferiority, withdrawal, self-doubt among Maori of New Zealand.
Zar
"possession" by Zar
spirits found in Ethiopia, Somalia, Chad, Niger & Egypt.
Usually affects
married women between 35 and 55 years of age.
Symptoms include: Fainting, insomnia, narcolepsy, constant headaches, heart palpitations, Stinging (pins and needles in extremities) depressant mood swings, digestion issues.
Treatments include use of Henna (hand painting), salt poultices, spirit possession ceremony.
Ceremony - Loud music & drumming, dancing, alcohol, slaughter of animal (blood to be consumed by possessed person) usually only women present.
Participants cuss, spit, drink, smoke, flirt, flail and express harsh opinions to help remove the Zar spirit.
Prognosis is that the person will likely have Zar spirit for life and will have repeating attacks.
Juju -
(Or KORO) Genitle shrinking in West African populations
CBC the current
Accusations of witchcraft and penis snatching in African
countries - March 25, 2013
Ogbanje / abiku - cyclical death and rebirth among west African Igbo of Nigeria (Ilechukwu, 2007)
Nakamura, Kitanishi, Miyake, Hashimoto & Kubota (2005) review
the neurotic versus delusional subtype of taijin-kyofu-sho.
This is a culture - bound syndrome of social phobia where individuals are obsessed with
how they offend others with their smell, behaviouors and presence.
Considering the diagnostic concepts of taijin-kyofusho (TKS) and social phobia they
compared the clinical diagnosis of TKS with the operational diagnosis of
Diagnostic and Statistical Manual of Mental Disorders (3rd edition, revised; DSM-III-R).
Found that overall 65.8% of 38 cases of TKS were diagnosed as social phobia
where the neurotic TKS cases were highest at 81.5% while delusional TKS cases were at 27.3%.
Additionally 42.1% of the TKS cases also were diagnosed with a mood disorder
where 60.5% of the TKS cases presented some axis II disorders. Those that did show
axis II diagnosis the most prevalent type was avoidant personality disorder at 31.6%.
Matsumi & Draguns Provide an overview of culture and psychopathology
They describe the nature of psychopathology and its diagnosis, including the biomedical model and the DSM categorization.
They continue to review a number of psychological disorders in cultural contexts, including: Affective disorders, Suicide, Schizophrenia, Alcoholism, Anxiety Disorders, Personality Disorders, Childhood Disorders.
The question of Cultural
Universals and particulars
arise with respect to emotions
and emotional experience.
Schacter-Singer: Two-factor theory - Requires cognitive appraisal and physiological arousal.
Cognitive interpretation of the physiological arousal is the emotion. ![]() Like going to the dentist
Like going to the dentist
Maranonon (1924) found with epinephrine: 29% felt emotion, but 71% felt 'as if' emotion.
Clearly some of these affective disorders vary across cultures, in spite of some measure of universality. Likewise, the experience of emotions also appears to have a core structure of common features, but a wide variation in expression and elicitation of emotional experience.
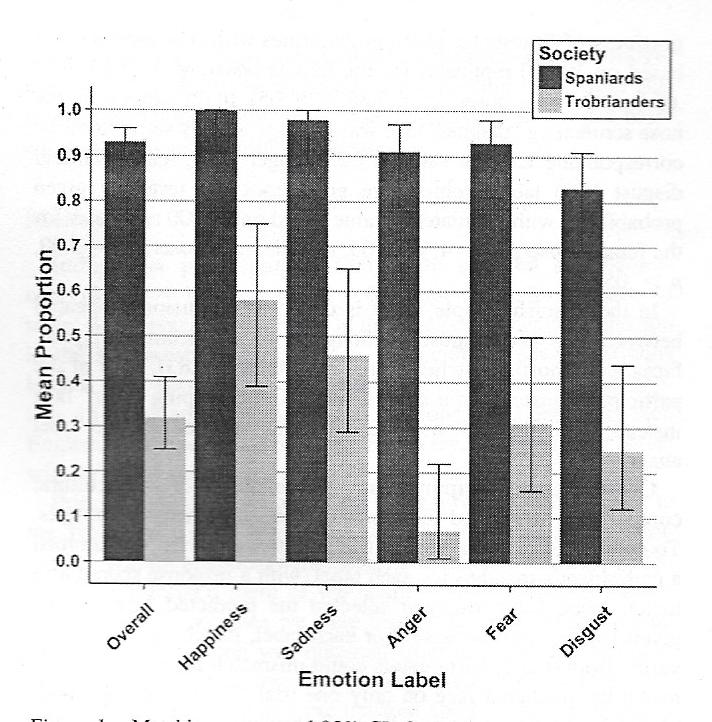
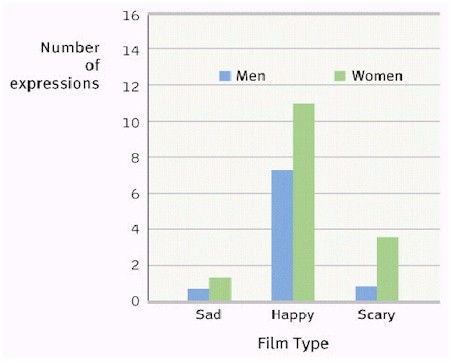
Emotional Facial Expression
Emotional facial recognition is performed well across cultures. There appears to be a basic biological set of emotion bases that can be mixed or altered into specific cultural emotions. ![]()
Recent work by Crivelli, Russell, Jarillo & Fernandez-Dols (2016a,b) shows that there is as little as Happy.58, Sad.46, Angry.07, Fear.31, Disgust.25 agreement with the facial expressions for Trobrianders and Happy1.0, Sad.98, Anger.91, Fear.93, Disgust.83 for Spaniards.
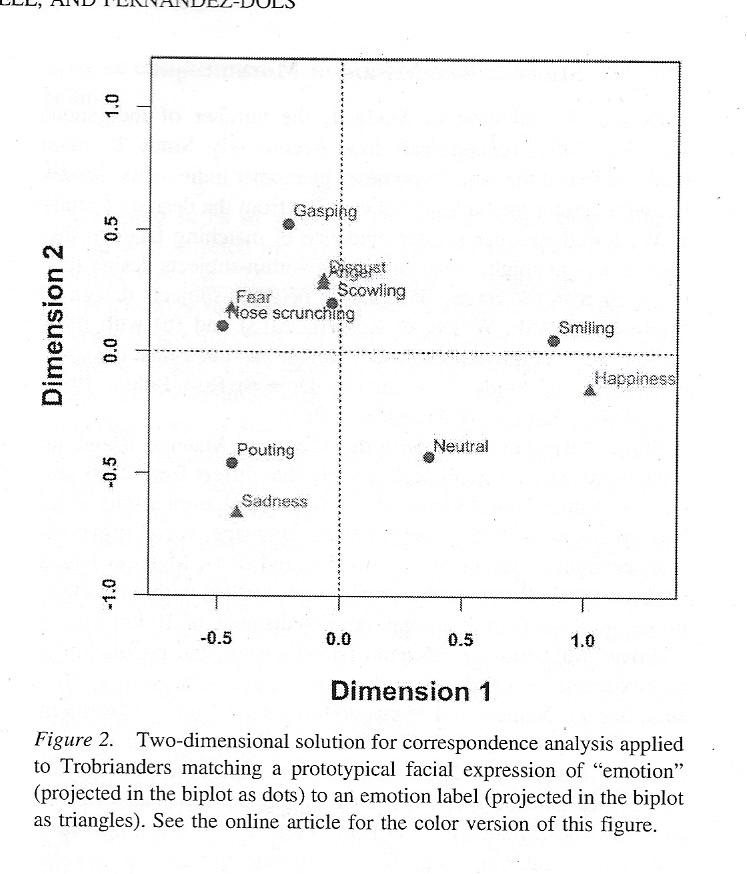
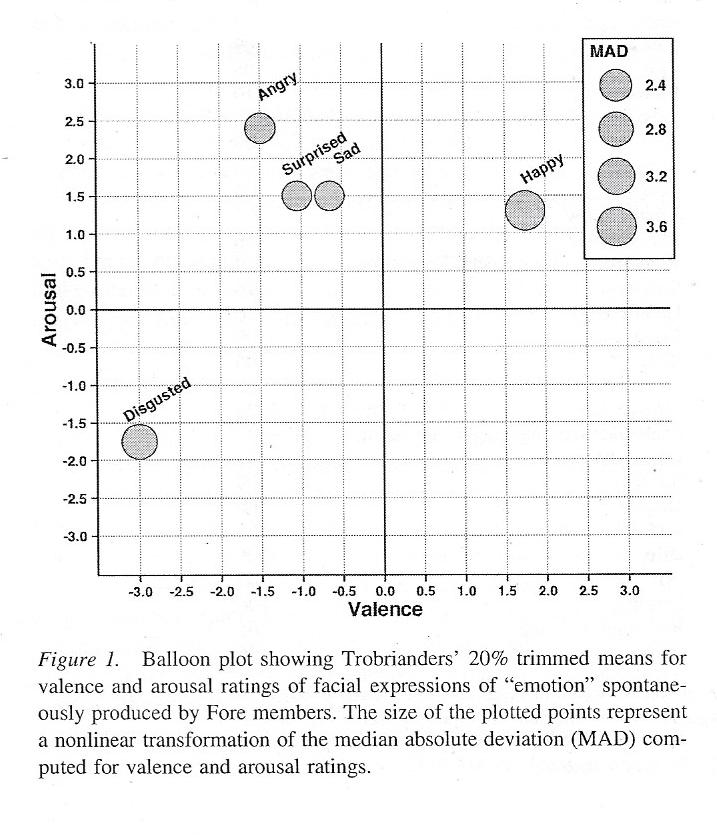
Likewise in comparing Trobrianders with others fro Papua New Guinea found:
Sad.16, Happy.13, Disgust.06, Anger.03, & Surprise0.0 for the correct identification of emotions in picture and Disgust.38, Sad.29, Surprise.21, Happy.17, Anger.13 in labelling of emotion faces.
They also found that Sad was often confused for Anger, Surprise and Disgust.
Lying and micro emotional expressions facial action coding
Catherine Lutz has examined emotional expression across cultures to consider the social construction of emotional experience and expression, i.e. Amae, Amok, ....Zazen.
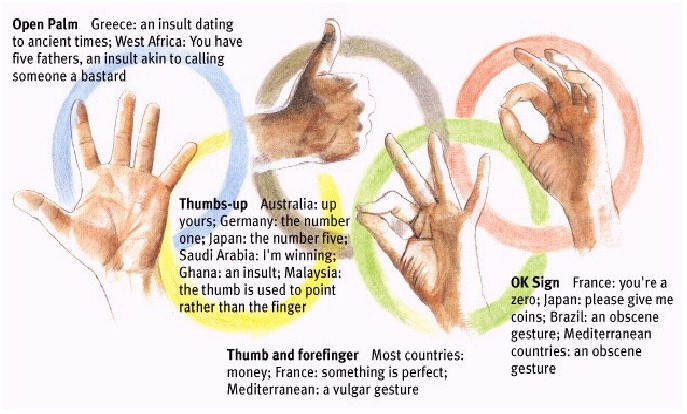
Display rules - pertain to how we show our feelings to others. These are unwritten expectations of how people should behave under certain circumstances. When at a birthday party or a funeral your emotions are expected to be of a certain form. With your teachers, parents or boss versus your friends and colleagues. Men & Women.
Nonverbal
communication and emotional state sensing depends on the gender
of people and on their familiarity.
![]()
Group activity - Examine various contexts of emotional expression in your lives and consider the role that social relations play in the feelings and behaviours as part of your emotional "syndrome" along with display rules for expression and experiences.
Counselling across Cultures
http://theashesofpersephone.wordpress.com/2009/04/12/zar-spirit-possession/
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}